

Aesthetic complication on a single lateral incisor implant
A 33-year-old female patient with no relevant medical history came to the clinic with the chief complaint of the appearance of her upper anterior teeth. Her lateral incisor 1.2 FDI (#7 US) presented mainly color and size asymmetry of upper anteriors and chipped left central incisor edge.
In the initial situation, she presents with agenesia and central incisors diastema. The patient underwent 3 years of orthodontic treatment and experienced retainer damage 1 year ago. She reports that her teeth were not on an even level. The patient has some composite fillings that are chipped. She also has a history of prior orthodontic treatment during her mid-late 20s to re-create space lost after tooth 1.3 FDI (#6 US) drifted forward and has had an implant to replace the right lateral incisor. The implant (Avinent 4.1 Coral Internal Hex) was placed under sedation at a previous practice in 2014. She has never been happy with the appearance of the implant crown and was left with a slightly misaligned upper anterior. The orthodontic retainer broke approximately 1 year prior to this consultation, but the patient was unaware of any tooth movement. She was anxious about anything related to the right lateral incisor 1.2 FDI (#7 US).
On the examination: An asymmetric smile was present with the right lateral incisor wider than the left lateral incisor. The midline shows a slightly left-hand shift. The right lateral incisor is flat, and the color, as well as the primary, secondary, and tertiary anatomy, could be improved. Gingival margins match the level of the upper anterior. The right lateral incisor papilla is at approx 20% of the clinical crown length, with the gingival translucency on the buccal aspect and a concave defect. The abutment is visible, as well as the transition to the crown.
Regarding the occlusion, the patient presents a static inter-arch anteroposterior relationship Class II Angle molar and canine on the right-hand side and a pseudo Class II on the left-hand side. Upper and lower teeth present some mild crowding. The upper dental midline is coincident with the facial midline, whereas the lower dental midline has deviated. The upper and lower arch shapes are triangular.
Evaluation & Diagnosis

Parallel occlusal and bipupilar plane. Minor imperfections seen on the incisal edge and color of the teeth.

Secondary dentition present except 1.8 and 4.8 (FDI). Implant crown present on the left lateral incisor (1.2 FDI).
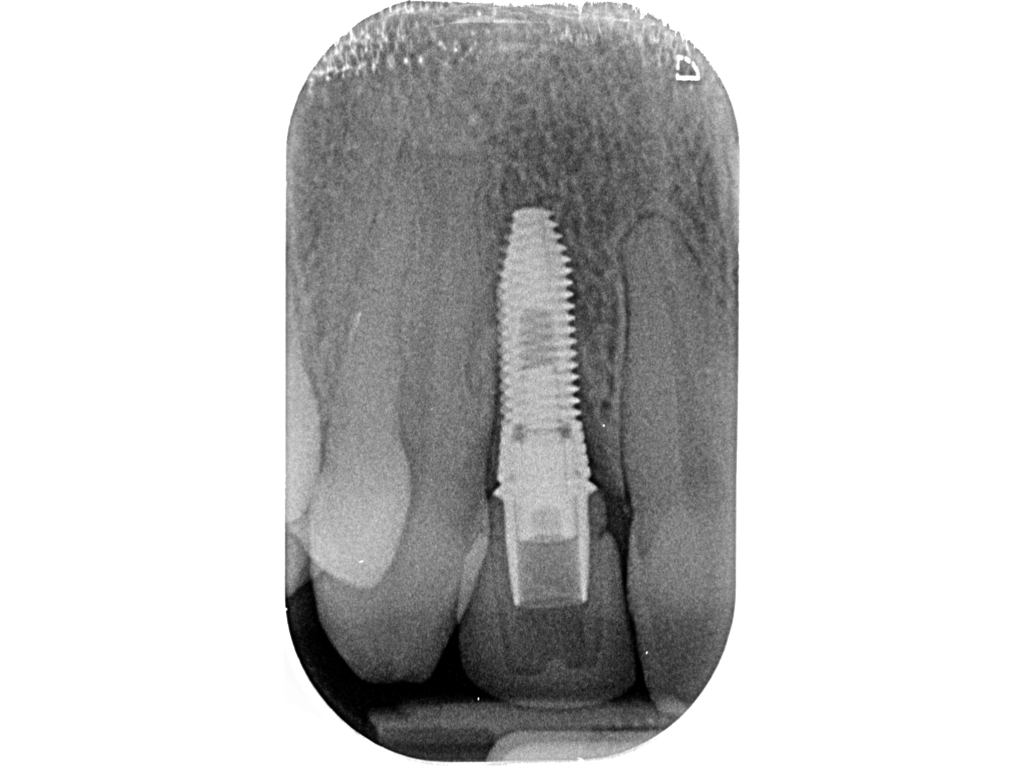
Implant ‘Avinent Coral 4.1 Internal Hexagon’ is in a subcrestal position towards 1.1 and 1.3 bone peaks.

Abutment/crown transition is visible and the shade match is not ideal with the grey translucency noticeable.

The maxillary right lateral incisor crown width is not proportionate in comparison with the contralateral tooth.

Upper anterior teeth in disharmony in position, width, shape, size, texture and colour.

Several defects on fillings noticeable in this view. Lower teeth present mild crowding.

Upper anterior maxillary teeth present mild crowding and first molars are mesially rotated.

Anterior teeth width are clearly assymetric. UL2 mesial filling defective. UR2 implant crown shows grey translucency.









Treatment Planning

Initial shade was close to A1 Vita Classic. Photo taken for lab communication.

A polarizing filter was used with a Reflex Camera and ring flash. Shade taken was performed with a Vita 3D Shade Guide.

Implant main axis is clearly buccal/outside of the ideal emergency by the zingulum area of the lateral incisors.

A screw retained provisional in with angle access driver allow us to tighten the restorations from the palatal aspect.




Initial treatment situation:
The situation was discussed with the patient, including the visible implant collar. The shape of the crown restoration is suboptimal, contributing to aesthetic deficiencies of suboptimal mesial-distal width, a papilla defect, and a buccal concavity. The complete arch space distribution, shape, alignment, and tooth anatomy were also considered.
The goals of the treatment were defined as follows:
-
Improvement of the teeth alignment and increase in the symmetric space distribution pre-restorative
-
Reduce the gingival translucency of the implant 1.2 FDI (#7 US) by providing more gingival volume
-
Improve overall aspect of upper anterior teeth of shade, shape, texture, and translucency of the upper anterior teeth
-
Orthodontic retention
-
Dental anxiety and phobia management
Two treatment options were discussed with the patient:
Option 1: explantation of the implant on the lateral incisor position, followed by a Guided Bone Regeneration and Connective Tissue Graft. This option could potentially result in a defect due to hard and soft tissue grafting.
Option 2: this option was considered to be less invasive as there was no bleeding on probing (BoP) present, no overall bleeding, and no suppuration, and the papillae could be preserved. The option included:
- 1.2 FDI (#7 US) temporary lab fabricated crown (as good as possible due to circumstances: immediate improvement in regards to mesiodistal width and shape)
- Connective tissue graft on 1.2 FDI (#7 US): at least 1 attempt, probably more would be needed
- Orthodontic assessment and treatment (the patient was happy with Invisalign Lite as it might be possible to include tooth whitening and retainers)
- Final implant crown on 1.2 FDI (#7 US) and a veneer on 2.2 FDI (#10 US). It was considered to place veneers on all upper incisors. In the end, the patient wanted to include the canines as well so as to make them appear smaller
Progress & Completion

After the orthodontic treatment, a satisfactory vertical, transversal and sagittal dental relatioships were achieved.

Some minor detalling could be improved, the patient wanted to stop the ortho treatment.

The 1.2 FDI over implant still shows some grayness and buccal concavity on the gingival margin.

Diastema between 2.2 and 2.3 FDI created for the final restorations to be more symmetrical and proportioned.


Lower dental midline is coincident with the lower lingual frenum insertion.

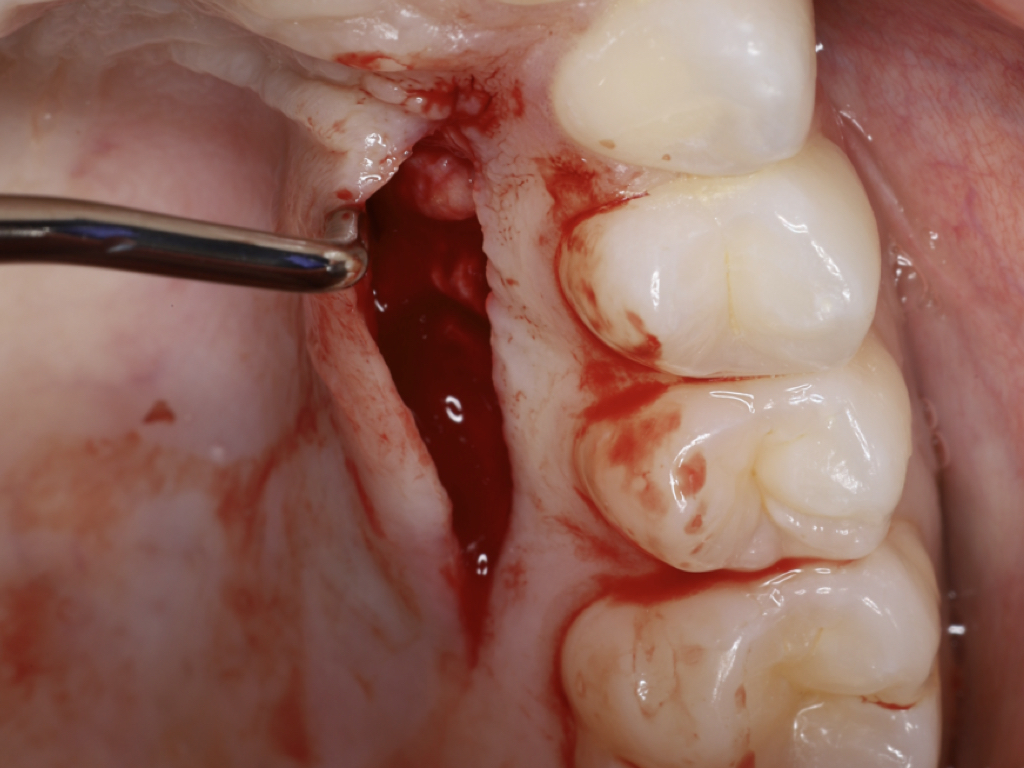
The buccal implant site on the lateral incisor area was prepared flapless with the tunneling technique.

It presents a size of about 15 mm long by 6 mm width and 2-3 mm thickness.

The graft was inserted and fixed into the recipient site by sling sutures.

Immediate post-op situation shows sutures mesial and distal of the implant to insert and fix the CTG in the pocket.
Coronal incision 3 mm from the gingival margin was extended from first molar to canine.

It was filled with a collagen cone and closed with 3 horizontal cross dental suspended sutures.

Smile analysis after ortho treatment and CTG.

Smile analyisis of the lateral view showing the diastema between lateral and canine.

Minimal preparations for eMax veneers. Inteproximal preparation will be hidden ffrome the eye sight with the veneers.

The implant area in the lateral (1.2 FDI) shows good gingival contour and the papilla are present.

Open-tray impression coping for analogue technique shows a good mesiodistal space distribution but buccally.

Open tray impression coping for analogue technique following the implan main axis is clearly buccal to the arch.

Shade record was taken after the teeth preparation.

Restoration filtting appointment situation after the provisional restorations removed and try-in of the Ti-Zr abutment.

Immediate post-op restoration. Minor cement excesses and bleeding are present.

Shows passive fit, narrower contour in comparison with the initial situation.

Good integration of the restorations pending to rehydratation of natural dentition for full evaluation.























The final restorations present good contact points and oval dental anatomy. The canine guidance is visible on the final lateral view.
Materials used:
Lateral incisor: Avinent Coral Internal Hex 4.1x with off-the-shelf abutment and Cerec crown. This crown was replaced by a temporary screw-retained crown with angle correction screw. The final crown was a cemented Emax crown on a Zirconia. The CTG was harvested from the palate.
- Orthodontic treatment with Clear aligners: Invisalign Lite. 3 set of aligners.
- Tooth whitening. Opalesence 16%
- Minimal prep eMax Veneers.
Follow-up & Outcome

Four weeks after restorations fitting, a frontal smile photo shows harmony, shape, position and color of the teeth.

The lateral incisor crown over the implant is well integrated with the natural dentition and restorations. .

Dental and gingival health aspect with integrated restorations and no greyness shining through lateral incisor.

Shows nice restoration adaptation with arch formation. Shade of the lateral incisor is reasonably integrated.

Shows good integration of the restorations including an increase on the papilla height on 1.2 FDI mesial and distal.

Shows excellent oral hygiene, periodontal and dental health.

Final photo with the polarizing filter shows great integration as well from the translucency.

This polarizing filter is used as quality control as well as feedback to the technician.








Conclusions
- A multidisciplinary approach needs to be considered even for a single implant case
- Less invasive treatments/alternatives are to be considered even when the existing implant position and size is not ideal, if the tissues are in healthy condition
- Different prosthetic tools could be used to compensate for a nonideal implant axis, such as angle correction screws or custom abutments for cementing
- The use of an opaquer to mask metallic abutments on temporary restorations could improve the aspect of these restorations. As an alternative, white or golden abutments might facilitate this task
- Soft tissue management and prosthetic design could lead to an enhancement of the aesthetics of the gingiva
- Space distribution, shape, texture and shade are important factors for a more natural result
Questions
Ask a question
What about the radiologic bone defects?
Obviously the esthetic issue was caused by an inadequate diameter of the implant, which was missplaced (buccal inclination) and insufficient restorative work out and insufficient materials in a thin morphotype patient. This caused radiologic bone loss and a shine throuh effect. You corrected the restorative parts very nicely and thickened the tissue by a connective tissue graft which did not keep its thickness (see follow up). This may be caused by bacterial biofilms on the implant surface and donor site selection (tuberositas area provide more stability). Do you think it would be helpful to clean the implant surface (GalvoSurge) first, augment the missing bone and simultaneously use a connective tissue graft?
Markus
Obviously the esthetic issue was caused by an inadequate diameter of the implant, which was missplaced (buccal inclination) and insufficient restorative work out and insufficient materials in a thin morphotype patient. This caused radiologic bone loss and a shine throuh effect. You corrected the restorative parts very nicely and thickened the tissue by a connective tissue graft which did not keep its thickness (see follow up). This may be caused by bacterial biofilms on the implant surface and donor site selection (tuberositas area provide more stability). Do you think it would be helpful to clean the implant surface (GalvoSurge) first, augment the missing bone and simultaneously use a connective tissue graft?
Markus

Dr Schlee, You need to flap elevation for GalvoSurge, don't you?

Dear Dr Schlee
Thank you for taking your time to review the case and your detailed question.
I totally agree on your views regarding the aethiology of the bone loss around the implant near to the platform mesial and distal, likely on the buccal as well. Also, I agree that the tuberosity would have been the first choice for the connective tissue graft for volume and stability. Possibly I decided to go for the palate to get lengths for the apico-coronal thickness boost but was not as successful as I would like to be. Due to the minimal gingival display after the lip filler and patient satisfaction, we decided to leave it as it is.
This case could have been approached in different ways including implant removal, hard and soft tissue graft and implant insertion at immediate or delay approach. Also, a good alternative is the one you were suggesting trying to rebuild the hard and soft tissues preserving this implant, for which, I would have use Galvosurge as part of the therapy.
However, as there was nor Bleeding nor suppuration on probing, no pocket depth >5 mm, patient reported no symptoms and a thin biotype was present. I decided to improve the main patient concern that was related to cosmetic as well as minimise risk factor due to the prosthetic design. For doing so, and as Dr Ozgur mentioned, the surgical treatment was flapless

Thanks to you to take the time to look into it

Thank you for presenting your case. The following are my questions and observations:
1. What is your solution, long term, for the lateral incisor?
2. How did you perform the connective tissue graft? Did you remove the abutment?
3. Did you raise a flap?
4. The final clinical situation is not stable in a young patient, What do you anticipate the changes are in a few years?
Best, Oded Bahat
1. What is your solution, long term, for the lateral incisor?
2. How did you perform the connective tissue graft? Did you remove the abutment?
3. Did you raise a flap?
4. The final clinical situation is not stable in a young patient, What do you anticipate the changes are in a few years?
Best, Oded Bahat
Dear Prof Bahat
I appreciate the time for your comments and observations. I will reply following the numerical order.
1. Unfortunately we do not know what would happen in the long term as she is 33 years old. There are few scenarios that I feel they are possible were either she might take the decision whether to keep or to extract the existing implant. With the current state of the art knowledge and the possibilities with new technologies we might choose to give a try to the periimplant tissue regeneration using Galvosurge and a combination of auto/allo and xenograft with a collagen membrane as barrier in a submerged approach.
if decided to extract the implant, a immediate post extraction implant with GBR and CTG if possible would be my chosen approach.
2&3. The surgery was done after removing the provisional implant crown to facilitate the technique. I performed flapless surgery with a pouch with tunnel to the adjacent teeth. A connective tissue graft was taken from the palate with a linear incision technique. Please, see the photos available.
4. if the patient continues with an excellent plaque control, I anticipate to be stable at least short-medium term. With age, patient might start having receding gum around teeth and implant.
Fortunately, there are few therapies on the armamentarium that would help boosting the biotype, from another connective tissue graft to buccal plate thicken with flap or flapless (VISTA, Pinhole)solutions.
I hope this answers your comments and happy to reply to any further ones
why veneer, you commit the pt to life long dental issues 6, 8-11, I can see #10 though
Why not Veneer? Teeth are treated with ortho and are in functional alignment. It both addresses cosmetic chief concerns and being minimally invasive. Done properly I’ve seen them last decades without issues and looking like the day it was placed.
Dear Dr Behar
Thank you for your valid comments.
I have to disagree to your statement that patient would have dental issues due to the minimal prep ceramic veneers. The life spam expected are minimum 15-20 years, they have been finished all in enamel and patient could benefit from new set of ceramic veneers if performed carefully.
On my hands and the cases I have seen, composite veneers do not perform very well unless done by a super talented clinician (it is not the case). Cosmetically and ageing is not brilliant and that would possibly condemn the patient to be in the dental chair modifying/redoing the treatment every 2-5 years.
On my clinical experience, I end up replacing a large amount of composite restoration due to faulty margins, morphology, fit and cosmetics.
I wish I could have that skillset but until Today with the technician I collaborate with, minimal invasive treatment with ceramic veneers outweighs the composite
My comment was regarding the implant, not your veneers. Please read my questions again. Your graft did not resolve the soft tissue challenge over the misplaced implant.
Best,
Oded
Dear Prof Bahat
Thanks for raising the issue about the buccal volume.
The veneer response was to Dr Behar comments. I did reply to your comments straight after your post, please, have a look. Also, further discussion has been done in answer to Dr Schlee comments.
Cheers
Javier
The single anterior tooth in a young female is the THE MOST DIFFICULT Rule out mental health issues or you are married to it
The solution here works, but something else might be done initially to just change the problem tooth number 7 (US). By utilizing a custom Zirconia abutment built on a UCLA abutment base, (if this implant system is compatible) you would have a white or shaded abutment and temporary crown to create negative space behind the gingival tissue at the implant base. Use a little more negative contour at the gingival mesial, distal and facial going below the gingival margin for both of these restorations. This will allow the gingiva to migrate up incisaly and gain some bulk even before trying to graft and then utilizing your contoured temporary for this initially over the abutment so # 7 will approximate the m/d emergence of number 10 more closely as shown in the original before photo. Once that has filled in after a month or six weeks or so, the patient can observe the results with the lighter tissue and tissue contour to the tooth to make a decision along with the doctor on what additional treatment would be beneficial.
How predictable is this option? It would not be more durable to explant, perform bone regeneration and connective graft.
The implant has been in function for 9 years now, no BoP, no SoP, no pocket >5 mm, gingival architecture preserved on the coronal area, no display on smile, very very anxious patient that cried in every and each appointment just talking about any work related to that tooth. ‘Primum non nocere’ what are the chances to have complications while explanting and vertical horizontal GBR on a thin biotype? Patient delighted with the outcome and less anxious about any treatment on that area. Certainly a non ideal implant size nor position with some bone remodelling. What is a prognosis of an extracted implant? What is the success rate over 40 years of an implant with a rough surface (she is 33 and expecting to leave up to 80)?
if all the answers were to be 100% success rate, go for it! I felt more reasonable to me to keep that implant that is full filling all the requirements for an implant from phonetics, to functional and cosmetic.
Dear Dr Almeida, I am afraid that the next photo is at the prep and impression stage

Could the implant have been masked with non resorbing graft materials like BioOss ?
In reply to Could the implant have been masked with non resorbing graft materials like BioOss ? by Anonymous
Can we see the outcome of the gingival graft ?
In reply to Could the implant have been masked with non resorbing graft materials like BioOss ? by Anonymous
Thanks for your comments
The answer is yes. A xenograft with DBBM on the buccal plate would have been a suitable option but in this case I decided to go flapless as per thin gingival biotype.
Unfortunatelly there are very little documentation of the surgical procedure or the post op follow up.