



Minimally invasive treatment a partially dentate elderly patient with dynamic navigation to place a tilted implant
An 80-year-old female patient presented with a fractured root on a distal fixed partial prosthesis element. Her case was solved with an immediate flapless implant placement using dynamic navigated surgery and immediately provisionalized implants mesially tilted.
Her relevant medical history reveals she is using anticoagulants and antihypertensive drugs. Over and above that, her dental history includes generalized gingivitis, localized periodontitis on tooth #1.5 FDI (#4 US) and recently, pain in the area of tooth #1.4 FDI (#5 US) due to a vertical root fracture.
In the clinical examination, she presents with tooth wearing in the lower jaw, a fixed partial prosthesis in the upper jaw, missing teeth #1.8, #1.7, #1.6, #1.4 FDI (#1, #2, #3, #5 US), and a fixed partial prosthesis over tooth #1.5 to #1.3 FDI (#4 to #6 US) with a distal cantilever of tooth #1.6 FDI (#3 US) restored almost 20 years ago. The patient has a bone quality type III and limited bone quantity due to the sinus position in the area of teeth #1.6 and #1.7 FDI (#3 and #4 US). Due to the vertical root fracture, buccal bone resorption on tooth #1.5 FDI (#4 US) is observed.
Evaluation & Diagnosis

Patient presents with a fixed partial prosthesis over tooth #1.5 to #1.3 FDI (#4 to #6 US) with a distal cantilever.

vertical root fracture and pain in the area of tooth #1.4 FDI (#5 US).


Surgical video
Progress & Completion

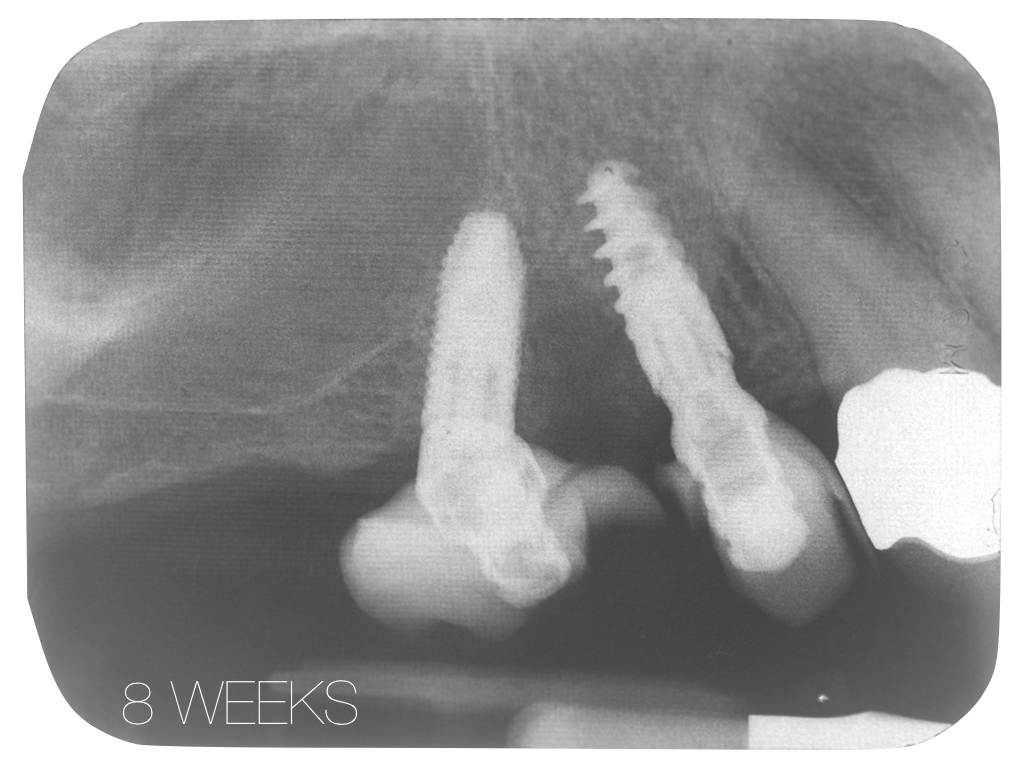
immediate implant placement in position 1.4 and 1.6 tilted mesially to avoid interference with maxillary sinus anatomy.

application of acrylic and polishing of the restoration to correct the critical and subcritical contours.

After 4 months, screw-retained CAD/CAM monolithic zirconia fixed partial prosthesis was performed.

at follow-up of 2 months using the provisional over implants.









Questions
Ask a question
Why use a Nobel Active and a Parallel CC
Question posted by moderator on behalf of FOR.org community member.
Question posted by moderator on behalf of FOR.org community member.
I used an active 3.5 in the 1.4 position so to have optimal primary stability and reduced implant diameter, in the position 1.6 I used a parallel 3.75mm diameter so to increase the mechanical resistance keeping the implant diameter relatively small. (Answer posted by moderator, on behalf of author, Dr. Luca De Stavola)
My plan would be as follows:
Separate the bridge from distal to the canine, and extract tooth the second bicuspid.
Then place 3 implants at the area of first and second bicuspid and short implant at the first molar area.
Then connect them all with one bridge.
(Comment posted by moderator on behalf of FOR.org community member)
Separate the bridge from distal to the canine, and extract tooth the second bicuspid.
Then place 3 implants at the area of first and second bicuspid and short implant at the first molar area.
Then connect them all with one bridge.
(Comment posted by moderator on behalf of FOR.org community member)
It is an option, in the area of the second bicuspid the bone was limited in dimension due to the infection around the tooth so I preferred to avoid the implant in that area an have the space to tilt the distal implant. (Posted by moderator on behalf of author, Dr. Luca De Stavola)
I have the following question related to the case (click on details):
A flapless immediate procedure was used to place implants,at # 14 and # 16 to replace failed FPD.I noticed no surgical guide was used clinically or confirmation of angulation and depth of pilot drill radiographically.Did I miss something or was it done freehand due to experience of the surgeon.Thanking you in anticipation. (Posted by moderator on behalf of FOR.org community member)
A flapless immediate procedure was used to place implants,at # 14 and # 16 to replace failed FPD.I noticed no surgical guide was used clinically or confirmation of angulation and depth of pilot drill radiographically.Did I miss something or was it done freehand due to experience of the surgeon.Thanking you in anticipation. (Posted by moderator on behalf of FOR.org community member)
The surgery was performed using the x-guide technology, so it was fully guided surgery but using a dynamic control of implant 3D positions. For these reasons no x-ray are needed during the surgery (Posted by moderator on behalf of author, Dr. Luca De Stavola)
Comment: New X-Guide workflow with X-Mark
X Mark is a great new addition to the X-Guide workflow. It allows me to virtually plan a case using the patient’s diagnostic scan and then accurately register the virtual plan to the patient for a predictable navigated surgery every time. No X-Clip in the scan means fewer appointments for the patient. (Comment posted by moderator on behalf of Dr. Robert Pauley.)
X Mark is a great new addition to the X-Guide workflow. It allows me to virtually plan a case using the patient’s diagnostic scan and then accurately register the virtual plan to the patient for a predictable navigated surgery every time. No X-Clip in the scan means fewer appointments for the patient. (Comment posted by moderator on behalf of Dr. Robert Pauley.)
Porque realizar una molar tan grande. Podría ser mejor biomecánicamente reconstruir con tres premolares
Abutment on #5
Hi
its a good case . Can u tell was a multi unit or what abutment was used on # 5
Hi
its a good case . Can u tell was a multi unit or what abutment was used on # 5